
How to contact VFRAC
Monday- Friday
Ph: 0481916095 OR fracturecare@wh.org.au
Resources:
WH Emergency Department Fracture and STI management guidelines (on prompt)
Virtual Fracture Clinic VFRAC (Adult) – PPG
Who are we?
Western Health is home to Australia’s first physiotherapy led Virtual Fracture Clinic which has been running since April 2017. This clinic is staffed by specialist Physiotherapists working in conjunction with Orthopaedic Surgeons to provide safe and timely care for patients after they have suffered a fracture or soft tissue injury. Western Health currently runs a Virtual Fracture Clinic service for both adults (VFRAC) and children (P-VFRAC).
What do VFRAC do?
- Advanced Practice Physiotherapists triage all WH ED referrals, and internal referrals to # clinic
- Triage simple patients independently, and discuss complex patients with a consultant
- Virtually manage patients with simple stable fractures and STI over the phone, including ordering repeat imaging if required
- Streamline care of patients coming to # clinic (eg. make sure they attend the right clinic at the right time, ordering imaging prior if capacity)
What is not part of the VFRAC role?
- Triage GP or external referrals (limited EFT)
- Manage complex patients (given phone only clinic)
- We cannot order CT scans/ MRIs – will defer to Ortho for this
Inclusion
- Adult patients discharged from a WH ED with a musculoskeletal condition (bony or soft tissue) appropriate for referral to the WH orthopaedic unit for management and not requiring immediate admission.
- ED referrals, and simple GP referrals triaged to VFRAC by Ortho
Exclusion
- Open fractures
- Clinical concern of neurovascular compromise
- Clinical concern of compartment syndrome
- Injury(s) sustained as a result of high velocity trauma
- MVA > 100km/h
- Fall from height >1m or 5 stairs
- Pedestrian or bike vs motor vehicle >30km/h
- Language and/or comprehension barriers to safe virtual management
- Paediatrics (<16 years of age) –> these go to Paediatric VFRAC
- Hearing impairment
- Declines phone management or no access to telephone
- Barriers to GP access
VFRAC Condition Triage & Management Guidelines
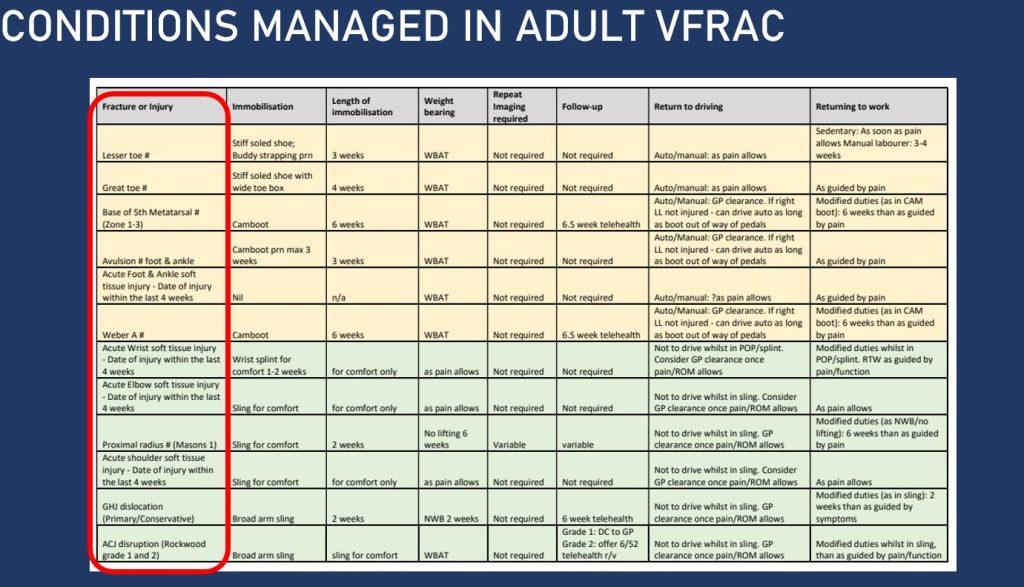
NB: Reviewed by Physiotherapy G4 Clinical Lead with Ben McElwee – May 2024
| Upper Limb | Shoulder | Clavicle fracture: – Undisplaced mid shaft – VFRAC x-ray at 6/52 (care plan) – Lateral or displaced – fracture clinic 1/52, erect clavicle XR on arrival ACJ injury: – G1 G2 – VFRAC, conservative management no follow up imaging (careplan) – Grade 3+ fracture clinic 1/52, bilateral ACJ erect XR on arrival GHJ dislocation: – Simple anterior – Vfrac follow-up, as per care plan. – Any other direction – discuss with Orthopaedics Fracture/dislocation – fracture clinic 1/52 (if dislocation confirmed reduction radiographically), erect shoulder XR on arrival – Recurrent dislocations – VFRAC manage via shoulder dislocation pathway – for MRI and Consultant clinic Other acute soft tissue shoulder injury confirmed on MRI (rotator cuff tear, labrum, etc): – discuss with Orthopaedics Scapula fracture: discuss with Orthopaedics – Proximal humerus fracture fracture clinic 1/52, erect shoulder XR on arrival – Head split – discuss with Orthopaedics Midshaft humerus fracture: – fracture clinic 1/52, humerus XR on arrival in immobilisation |
| Elbow | Distal humerus fracture: – discuss with Orthopaedics Elbow dislocation: – Simple – fracture clinic 1/52, elbow XR on arrival in immobilisation – Fracture/dislocation – discuss with Orthopaedics Radial head/neck: – Mason I Vfrac follow-up, as per care plan. – Mason II– Vfrac follow-up, as per care plan with XR 1/52 – Mason III – fracture clinic 1/52, elbow XR on arrival Olecranon fracture: fracture clinic 1/52, elbow XR on arrival Acute tendon rupture (radiologically reported) distal biceps – discuss with ortho | |
| Forearm | Monteggia injury – discuss with Orthopaedics Diaphyseal radius and/or ulna fracture – discuss with Orthopaedics Galleazzi injury – discuss with Orthopaedics | |
| Wrist | Distal radius fracture: – fracture clinic 1/52, wrist XR on arrival in immobilisation Distal ulna fracture: – fracture clinic 1/52, wrist XR on arrival in immobilisation Acute wrist soft tissue injury: – Vfrac follow-up, as per care plan. | |
| Hand | Distal radius fracture: fracture clinic 1/52, wrist XR on arrival in immobilisation Distal ulna fracture: fracture clinic 1/52, wrist XR on arrival in immobilisation Acut wrist soft tissue injury: Vfrac follow-up, as per care plan. Scaphoid fracture – Confirmed: fracture clinic 1/52, nil imaging on arrival – Clinically suspected: fracture clinic 10-14 days, scaphoid + wrist XR out of immobilisation Scapholunate injury: fracture clinic 1/52, nil imaging on arrival | |
| Lower Limb | Hip/ pelvis/ thigh | Isolated pubic rami fracture: Vfrac follow-up, no further XR, WBAT. Acetabular fracture: discuss with Orthopaedics Pelvic ring injury: discuss with Orthopaedics Any femur fracture: discuss with Orthopaedics Acute tendon rupture (radiologically reported) prox hamstring – discuss with ortho |
| Knee | PFJ dislocation: – Primary: fracture clinic 2/52, knee MRI prior to assess for osteochondral injury – Recurrent: discuss with Orthopaedics Patella fracture: fracture clinic 1/52, knee XR on arrival (AP + lateral + skyline) Meniscus – (updated post discussions with Scott Tulluch Oct 2023) – Acute suspected Meniscus no mechanical symptoms (undiagonosed knee)– GP with safety netting advice, investigations PRN – Meniscus true locked knee- # clinic – Meniscus confirmed < 55 years- # clinic – Acute Meniscus mechanical symptoms- # clinic – Confirmed Meniscus > 55 and no injury – discharge to GP – Meniscus > 55 and injury – VFRAC and GP follow upMCL/LCL MCL/LCL grade 1- VFRAC conservative MCL/LCL – MCL/LCL Grade 2 – VFRAC or Physio led ortho follow up – MCL/LCL Grade 3- consultant clinic ACL/PCL ACL – Confirmed ACL- consultant clinic – Suspected ACL (undiagnosed knee)- VFRAC/ d/c to GP with safety netting advice/ investigations PRN Confirmed chondral injury knee- consultant clinic Tibia: – Proximal tibia – discuss with Orthopaedics – Diaphyseal tibia – discuss with Orthopaedics | |
| Ankle | Soft tissue injury- No fracture and/or ultrasound or MRI reported medial or lateral ligament tears – Vfrac follow-up, as per care plan Syndesmosis – No fracture but MRI reported syndesmotic injury or suspicion – fracture clinic 1/52, WB ankle XR on arrival out of immobilization Avulsions (lateral mall, medial mall, talus) – Vfrac follow-up, as per care plan. Weber A – Vfrac follow-up, as per care plan. No repeat x-rays Weber B – fracture clinic 1/52, WB ankle XR on arrival out of immobilization Weber C, bimalleolar, trimalleolar, Maissoneuve – discuss with Orthopaedics | |
| Foot | Foot avulsion # eg. navicular, cuboid – VFRAC careplan Talus fracture (excluding simple ligament avulsions): discuss with Orthopaedics Calcaneus fracture: discuss with Orthopaedics Any other tarsal fracture: discuss with Orthopaedics Lisfranc injury or suspected: discuss with Orthopaedics Base of 5th metatarsal: – Undisplaced or min displaced Zone 1/2/3 – Vfrac follow-up, no further XR, WBAT in CAM boot for 6/52 – Displaced base of 5th MT- fracture clinic 1/52, WB foot XR on arrival Shaft of 5th Metatarsal – undisplaced- VFRAC with x-ray 6/52 if Ortho happy with position – displaced shaft- # clinic XROA Other metatarsal #: – Single – VFRAC as per base 5th careplan – Multiple – discuss with Orthopaedics Phalangeal (toes): Vfrac (care plan) Acute tendon rupture achilles – discuss with ortho | |
Authors and Contributions
- Phong Tran, Ben McElwee, Bhavna Trivedy, Sophie Gore – Nov 2024