
Introduction
The Enhanced Recovery After Surgery (ERAS) program aims to improve patients’ experience of care and expedite recovery from elective surgical procedures in the shortest possible time, without compromising safety and clinical outcomes.
The quality of the program is measured by:
- Safety (complications)
- Clinical effectiveness (outcomes)
- Patient experience.
- Cost efficiency of the program:
- Patient’s length of hospital stay
- Readmission rates to the hospital.
Aim
- Improve patient journey
- Optimise patients pre-operatively
- Decrease length of Stay
- Document and improve current processes
Williamtown LOS aim: 2 nights
Footscray LOS aim: 5 nights
Selection
Inclusion: All patients will be included in the ERAS THR/TKR pathway
Patient education and counselling
- Referral by GP
- Triaged to category 2 or 3 = waiting from 2 months up
- Initial consultant consultation
- Educating patients before surgery
- Aims and expectations
- Expected length of stay is specifically discussed and recorded in their consultation summary.
- Educating patients before surgery
- Patient reported outcome measures completed
- EQ-5D-5L
- Oxford Hip/Knee score
- Initial ERAS information given via information sheet
- Overview of ERAS
- Introduction to optimisation pre surgery
- Basic details around post operative mobility and pain management
- Details around discharge criteria and timeframe
- Waitlisted for surgery
- Category 2 or 3
- Campus suitability screening performed
Pre-Admission Clinic – PAC
Anaesthesia PAC
- Assess campus suitability, anaesthetic risks including those modifiable risks, or those requiring more investigation. Risk mitigation
Pharmacy PAC
- Obtain a full medication history
- Education regarding medication that may need withholding pre-operatively
- Highlighting any potential challenges or risks to the surgical and anaesthetic team
Surgery PAC:
- Screening investigations: FBE / UEC / LFT / coags / Fe studies / CRP / Hba1c, G&H, imaging, plus others as individually indicated (vascular studies, etc)
- Continue baseline opioids if patient is stable, attempt to wean if possible
- Diabetes assessment, medication advice (HbA1c if any DM diagnosis)
- Anticoagulant advice (withhold aspirin if primary prevention, continue if secondary. All others: discuss with registrar and cardiology / haem etc. Flag clearly for ward reference to help management of VTE prophylaxis / antiplatelets / other agents post-operatively)
- Hb optimization as per existing guidelines (HOBART guidelines)
- Smoking and Alcohol cessation – counsel in PAC
- Nutritional assessment – based on albumin (LFT’s). Below 30g/L must be flagged with surgical team, 30-35g/L needs minimum of nutritional counselling, and should be followed up closer to date if significant lead-time.
- Flag the high-carb drink (DEX drink) that is planned for day of surgery
OT PAC
- Obtain social history
- Obtain information about baseline occupational performance: cognition, personal, domestic and community tasks
- Obtain falls history
- Review of home environment, completing home assessment if required to aid equipment prescription post op
- Education about likely equipment or aids required post op, and Post-Acute hire/purchase options
- Total hip/knee replacement booklet given, and discussion about expected occupational performance post op
- Education about likely social supports and services required post op
- Set occupational goals required for discharge
Physio PAC
- Education about Day 0 mobilisation
- Baseline mobility assessment
- Goals for discharge.
- Discussing length of stay and planning for this
- Daily Goal sheet provided
- Advice about regular pain relief and cryotherapy post op to manage pain and swelling
- Recovery after Joint replacement surgery handout provided highlighting home exercise program – encouraged to begin pre operatively.
- Physiotherapy follow up discussed
- Discuss what type of clothing and shoes to pack for hospital to reduce falls risk
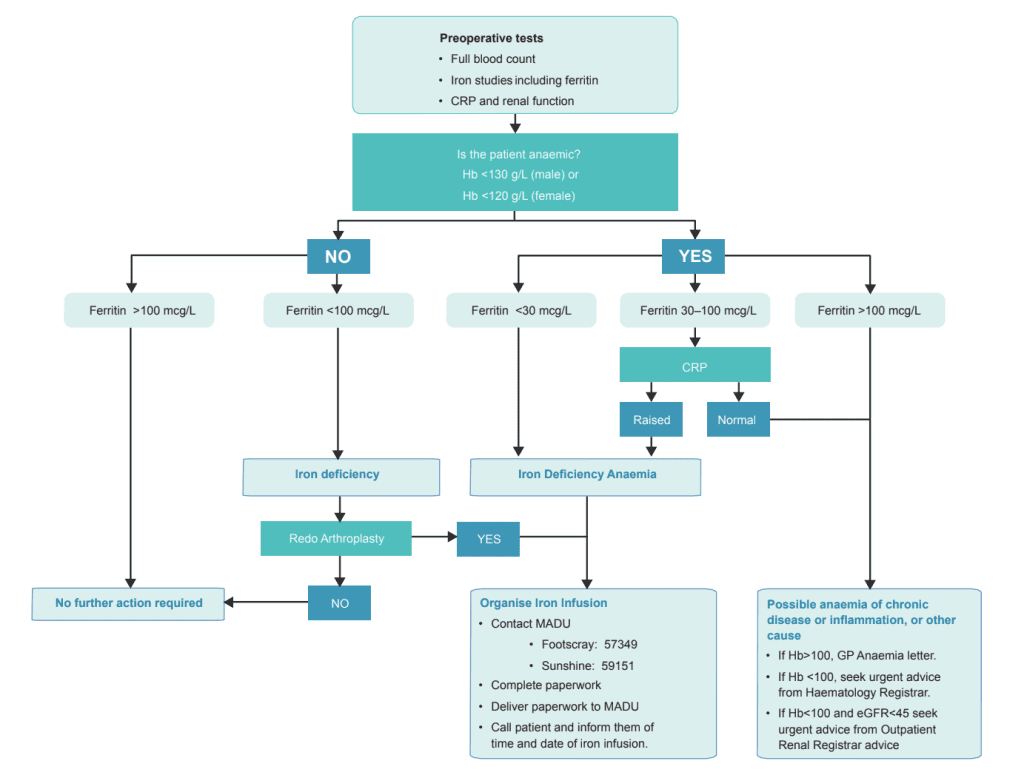
Anaemia screening:
- If patient is identified as anaemic, further investigations or management is triggered, as per Hobart protocol below:
Prehabilitation
- All patients who attend Pre-Admission Clinic are referred for prehabilitation
- Patients are managed via the endorsed Model of Care
- All patients are to attend a universal prehabilitation course which includes Virtual Surgery School (VSS) education sessions.
- The videos included in VSS are:
- Introduction to ERAS – add links
- QUIT smoking
- ACOUGH
- Psychology
- Exercise
- General Nutrition
- The videos included in VSS are:
- In addition to universal prehabilitation, all patients are screened for further targeted intervention for the following disciplines utilising the listed patient reported outcome measures:
- Physiotherapy – HOOS / KOOS
- Dietetics – BMI and MST
- Psychology – PHQ4
- Social work – Local screening tool
- Highlight the principles of ERAS regularly.
- Make patients feel that their care is individualised.
- Allow the opportunity for patient to access allied health staff and ask questions as needed
- All patient will repeat the above outcome measures as per the endorsed model of care if referral to additional disciplines is needed.
- At completion of prehabilitation all patients will complete the following patient reported outcome measures:
- EQ-5D-5L
- Prehabilitation patient experience survey
- Any discipline specific outcome measure which prompted targeted referral
Day of surgery
List ordering
- The patient is listed as an ERAS joint replacement
- Major joint patients should be listed first or second on a morning and all day list.
Peri-operative fasting and Carbohydrate Drinks
- The pre-operative fasting is minimised to reduce undue physiological stresses.
- Fasting from solid food for 6 hours pre-operatively
- Clear fluids can be taken up to 2 hours prior to surgery.
- High energy carbohydrate (DEX) drinks are given to all patients pre-operatively unless contraindicated
- Commonly used drinks contain 300kcal/200mls.
- https://www.dex.com.au/
Table 1. Fasting Instructions
| Morning List | Afternoon List | |
|---|---|---|
| Admitted | 0730 | 1130 |
| Eat Until | Midnight the day prior | 0630 |
| Drink Until | 0630 – have a glass of water / CHO drink | 1100- have a glass of water at this time / CHO drink |
| Pre op CHO drink | Before Midnight | Before 0630 |
| Post Op CHO drink | In Recovery | In Recovery |
* Water intake is then actively managed to reduce prolonged fluid fasting and dehydration.
Patient pre-warming
- Pre-warming is used routinely in the preoperative phase
- Patients are asked to wear conductive fabric or forced air warming blankets for pre-warming.
- There is good evidence that pre-warming patients results in reducing the risk of inadvertent hypothermia, which could result in coagulopathy with increased risk of transfusion, cardiac dysfunction and risk of infection.
Intraoperative Technique
- Preoperative
- Paracetamol 1g PO and Bair hugger in anaesthetic bay
- Anaesthetic:
- 1st line: Spinal +/- sedation + LIA
- 0.5% bupivacaine (heavy or plain) +/- fentanyl + IT morphine 100mcg for TKA
- LIA = 0.2% Ropivacaine
- <50kg = 60mL
- 50-70kg = 100mL
- 75-100kg = 120mL
- >100kg = 140mL
- 2nd line: GA+LIA+adductor canal single shot block (for TKA)
- Analgesia: Parecoxib 40mg IV (if eGFR >60)
- Antibiotic: Cefazolin 2g (unless allergy), if >120kg 3g
- Antiemetic: Consider Dexamethasone 4-8mg for nausea related to IT morphine
- Antifibrinolytic: Tranexamic acid 1g IV
- Fluids: Warmed CSL (aiming euvolaemia),
- Temperature: Bair hugger, Fluid warmer,
- Avoid IDC
- No PCA
- 1st line: Spinal +/- sedation + LIA
- Surgical
- Tourniquet: Per surgeon preference
- Surgeon placed adductor canal blocks for TKR
- Intra-articular TXA
Tranexamic Acid (TXA)
- TXA is utilised to minimise haemorrhage, by modulating clot breakdown. Under normal circumstances it is not associated with increased rates of VTE, cardiac events or CVA
- Anaesthetist – IV TXA dose is administered by the anaesthetist and is commenced prior to skin incision (1 g IV regardless of weight or renal function)
- Surgeon: intra-articular dose 1g post closure of the joint capsule
- A further dose of IV TXA may be given (1 g at least 8 hours after the initial dose) if deemed necessary by Orthopaedic team on post-op review – if there are significant concerns about ongoing haemorrhage e.g. high surgical drain outputs
Inpatient Management
- Encourage and enable patients to independently perform routine activities like eating, dressing and walking as early as possible.
- Patients are encouraged to take oral fluids in the recovery
- Mobilised on the day of the surgery, by physiotherapists but also by nursing staff.
- Regular ice-packs
Medication protocol
Analgesia:
- Order “Pain Assessment”, “Q2h while awake”
- This empowers staff to assess pain & offer analgesia frequently in the early post op course, as patient does not have the benefit of on demand PCA opioid analgesia.
- Paracetamol 1 g oral QID
- Celecoxib 100 mg or 200 mg (depending on age and renal function) oral BD
- Duration pain/function dependent, up to 1-2 weeks
- Consider reducing to single daily dose after first few days of BD dosing
- Tapentadol SR 50 mg oral BD
- Duration: 2 days for THR and 4-5 days for TKR
- Aim: to improve allied health participation
- PRN analgesia is the mainstay for dynamic pain & could be offered 45 mins before mobilisation
- 1st Line PRN:
- Tapentadol IR Q2H PRN
- Dose is age dependent
- Maximum dose in 24 hours is age dependent
- younger up to 600 mg
- Older 250 mg may be appropriate
- 2nd line PRN:
- Oxycodone IR oral Q2H PRN
- Dose is age dependent
- Oxycodone IR oral Q2H PRN
- TKR with insufficient functional gains due to pain severity
- Trial of anti-neuropathic – e.g. pregabalin low dose, may be appropriate for 1-2 weeks.
- Note: gabapentinoids are sedating & put patient at higher risk for falls
- Common side effects include: sedation, dizziness, confusion
- Dosage adjustment required with renal impairment: seek advice
- If anxiety is considered to be exacerbating pain experience:
- Note: gabapentinoids are sedating & put patient at higher risk for falls
- Trial of anti-neuropathic – e.g. pregabalin low dose, may be appropriate for 1-2 weeks.
- Trial of clonidine can be considered during admission if blood pressure allows
- Recommended starting dose: 50 microg oral BD or TDS
- Lower dose, of 25 microg, may be considered in small stature patient
- Short duration use would not require weaning (e.g. 2-3 days)
- Note: clonidine can contribute to sedation and hypotension, these risks must be considered before prescribing.
For further information please review: Intermittent Opioid Analgesia in Adults for Acute Pain and Associated Observations (Inpatients Only) PPG
Adjunct Therapies:
Prevent constipation
- Coloxyl with Senna 2 tabs oral BD
- Movicol 2 sachets oral BD (must be accompanied by good oral fluid intake)
- Lactulose 20 mL Oral BD PRN
Manage nausea/vomiting
- Ondansetron 4-8 mg oral/IV TDS PRN
- +/- Metoclopramide 10 mg oral/IV TDS PRN
- +/- Droperidol 0.625 mg IV Q8H PRN
- +/- Cyclizine 25-50 mg IV TDS PRN
Nurse practitioners are given the discretion to encourage patients to de-escalate analgesia as soon as possible.
Venous Thromboembolism prophylaxis
Total hips
- Mechanical: SCDs whilst in bed awake, no routine TEDs
- Chemical:
- Inpatient – Enoxaparin 20-60 mg subcutaneous daily, weight and renal function dependent
- Outpatient – Rivaroxaban 10 mg oral daily
- Total of 35 days duration including both Enoxaparin and Rivaroxaban
- Maximum of 30 days’ supply (PBS quantity) of Rivaroxaban on discharge even if patient received less than 5 days of Enoxaparin
Total knees
- Mechanical: SCDs whilst in bed awake, no routine TEDs
- Chemical:
- Inpatient – Enoxaparin 20-60 mg subcutaneous daily, weight and renal function dependent
- Outpatient – Rivaroxaban 10 mg oral daily
- Total of 14 days duration including both Enoxaparin and Rivaroxaban
- **Review clinical need for rivaroxaban if patient is also on other antiplatelet/anticoagulant agents**
Inpatient Physiotherapy
Post-operative physiotherapy usually commences on the day of surgery (day 0) for patients.
- Day zero mobilisation
- An initial assessment takes place approximately 2 hours after the patient returns from recovery.
- Mobilisation with appropriate support and gait aid
- Nurses have had training to ensure their competency in day 0 mobilisation.
- Discussing plans for a timely discharge
- Range of movement and strengthening exercises
- We encourage patients to use the limb normally, but not to force the joint into extremes of range until the soft tissues have healed.
- Educate around hip precautions as appropriate
- Progression of mobilization with an appropriate aid and transfer practice and stairs/step negotiation
- Cryotherapy
- Is commenced on removal of wool and crepe bandages to help reduce oedema and act as an adjunct to analgesia.
Inpatient Occupational Therapy
- In conjunction with nursing staff, facilitate patients to independently perform personal care tasks like toileting, showering, and dressing as early as possible
- Assess and prescribe ward equipment to allow for safe and independent management of daily occupations, such as long handled aids, shower chair and over-toilet frame
- Educate regarding the impact of any precautions on the performance of occupations
- Implement therapy to achieve or progress occupational goal attainment required for discharge
- Discuss plans for timely discharge and prescribe equipment required for discharge
- Complete referrals for any follow up Occupational Therapy
Discharge
All patients are given discharge information including follow-up appointments, prescriptions and contact phone numbers prior to leaving the hospital.
Patients are discharged as soon as the hospital discharge criteria are met.
Discharge Criteria
- Post-operative x-ray completed and reviewed
- Pain well controlled on regular oral analgesia
- Prescription completed with documented plan for analgesia weaning
- Patient has received medication counselling that includes a plan for recommencing medications stopped or withheld peri-operatively
- Tolerating oral intake
- Voiding urine without a catheter
- Satisfactory post-operative blood tests (U&E and FBC)
- Able to transfer / mobilise independently OR at a functional level appropriately and adequately supported for safe discharge home.
- e.g. home with family/supports able to provide supervision. minimal assist x 1 with aids
- Able to negotiate steps or stairs safely (if indicated)
- All occupational therapy equipment required for discharge provided
- Services/Care package in place (if needed)
- ERAS handout and follow-up provided
Discharge Medication
**Maximise non-opioids and preference atypical opioids**
- Paracetamol 1 g oral QID
- Celecoxib to complete determined course
- +/- Tapentadol SR to complete determined course
- PRN analgesia:
- Tapentadol IR 50 mg oral TDS or QID PRN
OR
- Oxycodone IR age-based dose 2.5 mg / 5 mg / 7.5 mg / 10 mg oral TDS or QID PRN
- Supply quantity (usually 10-20 tablets, no repeats) is dependent on PRN requirement in previous 24 hours, patient’s age and accessibility to GP or medical services during the expected recovery period (e.g. may require more doses in times of public holidays)
- Tapentadol IR 50 mg oral TDS or QID PRN
- Laxatives:
- Coloxyl with or without senna, 2 tablets oral BD
- AND
- Movicol 1-2 sachets oral daily
- Continue for 2 days after regular or PRN opioids are no longer required
- Coloxyl with or without senna, 2 tablets oral BD
- +/- anti-emetic PRN – check with patient if required
It is clearly explained to patients that opioid analgesia is for short-term use only and may not be continued by their GP once the courses are complete.
All patients are given discharge information including follow-up appointments, prescriptions and contact phone numbers prior to leaving the hospital.
Postoperative Management
Post-Operative Wound Care
Patients are educated to leave the occlusive dressing intact and to present to ED rather than seeking GP care in the first instance.
Wound review is performed at 2 weeks, with a brief assessment of functional gains since discharge.
- Within catchment:
- Referred to Post-Acute Care via Bossnet Community services referral
- Outside of catchment:
- Referred to outpatients via EMR
Challenges or gaps in post-op care can be addressed here.
Outpatient Physiotherapy
All patients are discharged with exercise advice (booklet format) and contact information
**Insert documents**
Routinely all total hip and knee replacement patients are referred on discharge with request for an appointment approximately 7-10 day post-op at a hospital closest to where they live.
Orthopaedic Follow–up
The patients are seen in the outpatient clinic at six to eight weeks post-op for clinical assessment.
Referral for this is made at discharge via EMR
Further review is tailored to the individual patient based on progress.
Patients making satisfactory progress are discharged at this point or are given an appointment to be reviewed again at the anniversary of their surgery.
Updates and Presentations
September 2023 – ERAS Sustainability
To Do
- Update Orthoanswer
- Make the program sustainable
- Increase ERAS to other procedures
- Import ERAS dataset into Sunray and make collection of this data – standard of care
Authors
- Rebecca Fewster (2023)
- Phong Tran (2023)
- Sean Griffiths (2023)
- Lily Salehi (2024)