
Stakeholders – PAC NUM, HMO, Registrars, Anaesthetist, Surgical Bookings
The Western Health Preadmission Service operates over 2 campuses – Sunshine campus & Footscray campus supporting elective surgery to ALL campuses in Western Health.
The clinic operates between: 0830 – 1700 hours each weekday. It is closed on weekends and public holidays.
Preadmission Clinic Schedules
Generic Nurse Led Phone PAC
- Mon – Friday 0830-1700 with an AM and PM lists
ORTHO UNIT clinics (Face to Face or Telehealth/Telephone)
- Footscray: Monday 0830 -1230 and Thursday 0830 – 1230
- Sunshine: Tuesday 0830 – 1230
- These clinics run with PAC Nurse, Unit Doctors (Interns or HMOs) and major clinics with Anaesthetist support in clinic
Staff
NUM: Suzannah Beasely, Suzannah.beasley@wh.org.au
PAC Health Assessment Team Comprises of:
- PAC Nurses.
- Surgical Unit Medical Staff – Interns/HMOs, occasionally Registrar
- Anaesthetists – in designated clinics
- Perioperative Pharmacists (Major PACs only)
Each Pre-Admission (PAC) clinic has 3-4 nurses & 1-2 doctors (Interns or HMO) attending depending on the clinic.
The larger clinic appointment templates (> 8 time slots) are arranged for at least two doctors to attend from each unit.
- Please be prompt at attending – A.M clinic: no later than 0930 hours, & P.M. clinic: no later than 1330 hours.
- If you are on your own due to staffing issues, ensure to ask for assistance from any available colleagues early, especially if it is a major clinic.
CONSULTANT ANAESTHETIST (or Registrar)
Sunshine (Allocations subject to change depending on Anaesthetist availability)
- An Anaesthetist can be allocated to a major surgery PAC clinic.
- There may also be a separate Anaesthetic list running concurrently for File Reviews and other Anaesthetic patient reviews.
Footscray (Allocations subject to change depending on Anaesthetist availability)
An Anaesthetist is allocated to major ortho PAC clinic on Thursdays.
You can ring the Anaesthetist In-Charge in theatre at the campus to discuss the patient’s needs or for advice on days they are not in attendance at PAC. The contact number for the In-Charge Anaesthetist at that campus is on the white board.
Aims of Pre-Admission Clinic
Elective surgery adult patients may receive a Pre-Admission assessment prior to surgery. This can be done either in clinic as a face to face assessment, or via Telehealth/Telephone review. For minor cases, these may be suitable over the phone by a PAC nurse.
Preoperative assessment establishes that the patient is fully informed and wishes to undergo the procedure. The aim is to ensure the patient is as fit as possible for the surgery and Anaesthetic and is safe to proceed.
- Optimize the health of the patient, identify any risk factors prior to the admission date and to ensure the patient proceeds to surgery in a safe and timely manner at the appropriate hospital campus. (see Campus guidelines on intranet under Anaesthesia and Pain Medicine)http://inside.wh.org.au/policies-procedures-forms/WHDocuments/Appropriate%20Campus%20Selection%20for%20Patients%20Scheduled%20for%20Surgical%20and%20Endoscopic%20Procedures.doc
- Confirm the need for surgery through interview and only if required; physical examination.
- Provide both pre and post-operative education to the patient. This may involve other members of the multidisciplinary team at some stage e.g. Occupational Therapists and Physiotherapists.
- Ensure the consent is Valid and patient understands the procedure they are having and has done a fully informed consent. This includes the use of Interpreters or Medical Power of Attorney to co-sign, and the correct procedure, procedure written in full and clear, surgical site/side, signed by Doctor and patient and dated. Consent is valid for 12 months.
- Order and follow up on any pre-operative tests required. e.g. Blood & urine pathology, Medical Imaging, specific tests
It is the Surgical Unit’s responsibility to follow up any results from Pathology or Radiology that are requested in a UNIT PAC. This is done as part of PAC Follow Up.
Any Cardiac or Respiratory test results after PAC can be reviewed in Clinic by an Anaesthetist as an Anaesthetic File Review (ANAES F/R).
Inform your Surgical Unit’s Liaison Nurse (SLN) from the Elective Surgery Bookings Office of: any updates, deferrals, change in status, etc. which occurs outside of a completed PAC. Make any additions to your PAC notes as an addendum to that episode’s PAC Admission note.
** It is the Surgical Unit’s responsibility to inform bookings of any changes to a patient’s
Ready For Care status once PAC has been completed after the PAC appointment day**.
Other Staff associated with PAC:
Orthopaedic – Occupational Therapist: The OT ensures that patients undergoing major joint replacement surgery are prepared both pre and post operatively, allowing time to assess physical and social needs and any requirements for post-operative rehabilitation. These appointments are done by OT in the background.
How the Preadmission Clinic Operates
Abbreviations: dMR = Bossnet. EMR = EMR (Cerner). SLN = surgical liaison nurse
- Since COVID, PAC is predominantly run as a phone-call/tele-health clinic.
- On the left is a whiteboard with the patient’s names: they are either for a complete PAC (go through the entire series of pre-op questions; follow a template), or a file review, meaning someone has already completed the PAC, but something needed chasing up. Pick up the next patient from the list, write your initials on the whiteboard and complete your pre-admission clinic review.
- Once the patient r/v has been completed – cross through your tick on the board. Then, place the paperwork in the next tray/slot for r/v (e.g. for Anaes) or if everyone has seen the patient, place in the Completed Tray.
- If using an interpreter, be mindful of interpreter’s timeslot and ensure reviews by different clinicians are completed consecutively.
- Patients are generally seen by the PAC Nurse first who will complete a Health Questionnaire:
- Please direct any questions you have regarding the patient to the nurse that saw the patient
- The nurse health assessment is completed on the PAC Nurse Health Questionnaire on EMR; admission details if known are confirmed with patient and a set of vital signs are taken (if face to face). On EMR find under: Case Conference -> PAC Nurse HealthQ & name of surgery, in title of document.
- The nurse will attempt to also source any reports or correspondence from GP’s, other hospitals etc.
- At the top of the Health Questionnaire is: ‘PAC Assessment and Procedure Summary’ section that is also completed by the PAC nurse.
This section includes the:
- Routine: The surgery, Surgeon’s name, Category, Date (if known), Length of Stay, Consent Validity etc.
- Subheadings: Assessment and Unit or Anaes R/V are included where the nurse will make a note of any Path or Imaging available or requested
- Concerns or issues to be addressed such as: anticoagulants, high BMI, campus suitability, other health issues to address, pre-op requirements that need ordering etc.
- Please check the information on the Health Questionnaire. Ensure your own assessment aligns with the information on the Questionnaire.
- The Consent is checked to ensure that it is on the DMR, completed correctly and legally and the patient has ‘informed consent’ i.e. signed by patient & consenting doctor and dated & co-signed by approved interpreter if non-English speaking or Medical Power of Attorney (if appropriate).
- Anomalies will be recorded in the Summary section on the Nurse Questionnaire for the Unit to action.
- If applicable, the nurse will do an ECG (if patient face to face) where appropriate, according to Anaesthetic guidelines.
- The Consent is checked to ensure that it is on the DMR, completed correctly and legally and the patient has ‘informed consent’ i.e. signed by patient & consenting doctor and dated & co-signed by approved interpreter if non-English speaking or Medical Power of Attorney (if appropriate).
Please sign off any ECG’s before the patient leaves. It is your responsibility to address any issues in your surgical plan.
- If the patient has already been flagged for an Anaesthetic review, we will mark this on the board with an asterisk (*) under the Anaesthetist column. Depending on who is free, the patient may see the Anaesthetist or the Unit doctor after the nurse. If you feel the patient needs to see the Anaesthetist, and is not already flagged, please flag this on the white board with an asterisk.
The other option is a discussion with the Anaesthetist and no formal review. In this case please indicate this on the whiteboard with a D/W and √, so the PAC staff is aware the patient does not need to stay for a face to face review or have a telephone review with the Anaesthetist.
Please document this discussion, name of Anaesthetist and any advice given to the patient in your notes.
Anaesthetic Review
Patients undergoing major surgery and/or have major co-morbidities that may affect their outcome or recovery, will be seen by the Anaesthetist. The Anaesthetist will document their assessment on the PAC Anaesthetic e-form in EMR. Their role is to assist in deciding campus suitability, discuss different types of anaesthesia with the patient, aid in decisions regarding patient’s anticoagulation, medication advice, and possibly defer the patient if they feel further investigations are necessary.
Please ensure you read the Anaesthetist notes if you have seen the patient first. This is to make sure that any information given to the patient is the same from all parties. e.g. anticoagulation advice. This goes both ways and the Anaesthetists are also encouraged to engage with the HMOs.
Surgical Unit HMO Review
It is the role of the intern or HMO in PAC (on clinic day) to ensure the patient is aware of the surgery that they are having and to ensure that all the relevant unit based investigations have been completed. We have standard requirements for different investigations depending on the procedure planned and as per the Anaesthetic guidelines. Please use your unit handbook and PAC guidelines and advice from your senior colleagues as to what you should be ordering.
Anaesthetic guidelines for Ordering Basic Pre-Operative Investigations. http://inside.wh.org.au/policies-procedures-forms/WHDocuments/Guidelines%20for%20Ordering%20Basic%20Pre-Operative%20Investigations.doc
Most PAC guidelines are available on the intranet under either Pre-Admissions or the Anaesthetic Dept. There is also a current copy of the Unit PAC guidelines in the consulting rooms. Please copy for your own use – Do not write on, or use the original or remove from the room.
Ask the nurse in charge of the clinic if you are unsure it’s the current version. There are also copies of other Anaesthetic and diabetic guidelines in the rooms in a folder.
- Pre-operative Guidelines for OSA, Diabetes, Campus suitability, Anticoagulant guidelines etc. are in the Anaesthetic Department section on the intranet.
- Some investigations may have already been done externally, if relevant these will need to be requested either by yourself or the PAC Nurse so they can be scanned into DMR. Occasionally pending results of these investigations are the reason patients are made NRFC and therefore ensure a Unit or Anaes F/R is booked, so the patient is not lost to follow up.
Pre-admission Surgical Unit Notes on EMR
- Please use the correct PAC ‘Admission note’ template.
**Create Note: Admission H&E – This will self-generate its own sections including medications. These sections can be modified as required.
- All PAC-associated notes should be on the Pre-Admission Admission Note – see the QRG PAC: JMO Admission Notehttps://digitalhealth.wh.org.au/wp-content/uploads/2019/06/Pre-Admission-Clinic-JMO-Admission-Note.pdf
- The Title of the Admission Note follows the Naming Convention: PAC ORTHO ADMISSION PROCEDURE
e.g. PAC ORTHO ADMISSION RIGHT TOTAL KNEE REPLACEMENT
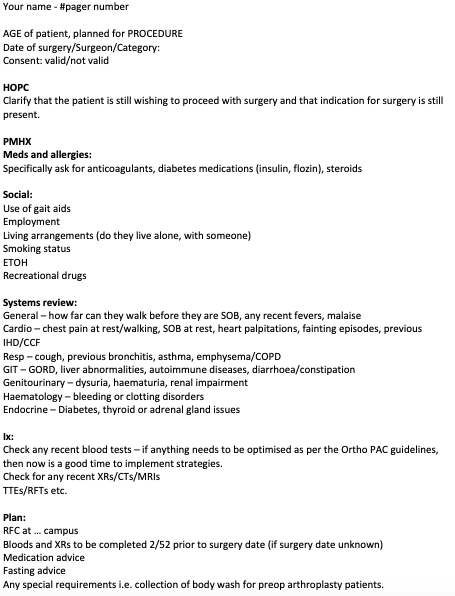
- Below is an example of a template for PAC that you may find useful
- All further notes from that PAC episode e.g. follow ups, discussions, further advice etc. can be written on the same PAC episode note as an Addendum. This keeps all records for that episode of care together.
Pathology Requests
Please ensure that all tests/investigations that are ordered are considered, and relevant to the procedure and to the patient’s pre surgical condition. If relevant pathology has been done previously and is still current within 3 months, please do not re-order same tests, unless they have been abnormal. Tests are expensive so please do not over order. Patients are to complete all pathology and imaging at a Western Health campus if they live in standard Western Health Catchment. For the truly rural patients, be considerate but realistic – G&H cannot be accepted if done elsewhere, and if the PAC team arrange for investigations to be done externally, it is your responsibility to bring them into Western records pre-operatively.
If unsure of Pathology request process, please speak to the Nurse In Charge or ask your registrars.
It is the surgical Unit’s responsibility to follow up any investigations ordered in PAC. If an abnormality is detected, consider the patient’s baseline, any contributing factors or risks that this may pose to their successful recovery post-operatively, and discuss with the registrar on the list (if allocated), or the on-call registrar (if not yet scheduled).
Baseline Pre-operative Pathology Testing
- Surgical Liaison Nurses
- The Pathology investigations that you order in PAC are generally considered a snap shotof health at PAC and are relevant for at least 3 months unless their condition has changed in that time.
- Please ask patients with a surgical date to attend for all their baseline investigations on the day of their PAC appointment (if face to face), or soon after their PAC appointment where possible.
- If attending F2F, can attend on the day of PAC at the hospital Pathology Collection centre. You can then follow up in a timely manner pre-operatively.For those done via Telephone/Telehealth, please arrange with patient best way to get the request slip to them; e.g. patient’s email, email to the Hospital Pathology collection centre and attend, or take in person to the nominated hospital Pathology collection room for them to come in during the week. (Footscray Hospital or Sunshine Hospital Dorevitch collection centre)
- Document in your Plan what Pathology tests (+/- ECG) have been ordered, and the arrangement made with the patient and where the requests slips are, or have been sent.
- Regarding Joint replacement patients, Elective bookings team will organise pre-op blood tests and ECGs on behalf of the unit 2 weeks prior to surgery date. PAC resident will need to chase those results and notify registrar responsible for the list if any abnormalities detected
- Please ask patients with a surgical date to attend for all their baseline investigations on the day of their PAC appointment (if face to face), or soon after their PAC appointment where possible.
e.g 1: FBE, EUC, Coag, ECG & Ext G&H – request slips emailed to JohnSmith@xmail.com. Pt will do baselines this week. Awaiting surgical date- will do Ext. G&H within 2/52 of surgery date at WHF Path. Slip in FPAC Path tray for collection.
e.g.2: FBE, EUC, TFT, ECG – Request slip given to patient, will do today at WHS Path.
e.g.3: FBE, EUC, Coag, ECG – Request slip emailed to WHS Path, Patient will do within 2/52 when given date. Copy in of request in SPAC folder.
Group and Holds:
- All patients requiring G&H from PAC, if eligible, can have an ‘Extended G&H’ requested. This can only be ordered from PAC and on a PAC Path form with a PAC clinic Bradma.
- An Extended Group and Hold expires after 30 days (blood is held for 30 days)
- For this to occur it is extremely important that when filling out the G&H form you ask the patient the questions on the right hand side of the form, in the box.
- To be eligible for an extended G&H, patient must answer NO to all those questions. A common occurrence in PAC is a patient who has had a blood transfusion within the last 3 months and therefore will be ineligible for an extended G&H – ensure you check the health questionnaire & ask the patient. If ineligible, they will require a G&H to be taken <72 hours prior to surgery.
- If you do not complete the G&H form correctly, Blood Bank staff may page you to come and complete the information
- Exception to an ‘Extended’ G&H: are patients that have had a recent blood transfusion or known antibodies. Check the Health questionnaire & ask the patient or check previous G&H results. These patients will require G&H < 72 hours prior to surgery. In this case a separate G&H form can be given to the patient to attend <72 hours prior to operation. Note: All other baseline pathology can be done on day of PAC or week of PAC for those without dates
- In each room you will find a helpful list of what surgeries generally require a G&H and those that do not. Please use this; it is a good reference guide. A cross match is not necessary unless clinically indicated or the patient has known antibodies, in which case pathology will alert the Unit to this once the G&H is done, and the patient will be ineligible for the ‘extended’ group and hold. The patient will then require a re-bleed <72 hours prior to surgery with 2 units cross matched. You may be required to organize a re-bleed.
Group & Hold requests can only have blood collected at Footscray or Sunshine Hospital Dorevitch Pathology, not at external Dorevitch collection centres or at Williamstown Hospital.
Pathology for Patients Without a Surgical Date:
Baseline pathology may be done on day of PAC e.g. FBE, UEC, COAG etc. as mentioned above. No need to wait until patient has a date. Remember, it’s considered a snap shot of health at PAC.
If the patient requires extended G&H also, this expires after one month. Please ask the patient to do the baseline Pathology on day of PAC or during the week, so this can be followed up.
- If a G&H is also required, provide the patient with the separate G&H request and instruct them to do the G&H 2/52 prior to their surgery once the Elective Bookings Office allocates a confirmed surgical date. Once these patients are allocated a date: the patient will need to write the campus and date on the G&H form. They can fill this part in, or tell the Pathology collector the date and campus.
- Please note this in your Plan along with what tests you have ordered. If review done by Telehealth/Telephone, please note where you have sent the request forms and any instructions you have given the patient. (See examples mentioned above in Baseline Pre-operative Pathology)
Pathology & Expired PACs:
If a surgical date is not given within 12 months, the PAC may expire and the patient may need to have a PAC review again, or if their health or medications have changed. In this case, new Pathology can be ordered at time of new PAC.
Patients who have previously had a PAC that do not need another PAC, may need new Pathology/Investigations organized by the Surgical Unit. In this case, the Surgical Liaison Nurses from Elective Surgery Bookings Office may just inform the Unit of the date of surgery. The surgical Unit should follow up if anything further needs organizing preoperatively.
- Elective Surgery bookings Office should notify the Unit when the date is allocated to ensure Pathology/Investigations are followed up pre-operatively. Your Unit may have a designated person to check pre-operative lists. Your Unit’s Surgical Liaison Nurse (SLN) is your contact point to ensure information is passed to Bookings and vice versa.
PAC Review Completed
Please make sure you have completed all your notes and you have written a Plan in your notes. Ensure you refresh EMR so completed notes can be seen by other staff. The note should be marked as ‘Final’ not Preliminary. We should not see ‘Preliminary’ notes – please do not write notes until you actually review the patient. If you wish to research/reconcile information prior to PAC this can be done separately on a word document or notepad and the information transferred to the EMR Admission note, once you speak to the patient.
The Plan should include:
- Proceeding to surgery (fitness) and campus’ suitability (not just where currently booked). Please include all campus’ where the procedure could be done.
- Investigations ordered, Pathology tests requested (indicate which tests) +/- ECG and arrangement for request slip and attendance.
- +/- ECG: reviewed & signed off before patient leaves, or if requested.
- Anaesthetic r/v or discussion – please indicate Name of Anaesthetist and advice.
- Any discussions with other surgical staff, Consultants, Registrars, other teams.
- Any follow up required outside of PAC. e.g. follow up with patient’s GP ensuring a chest infection has cleared, ensuring external radiology reports/scans received etc.
Once the PAC is completed by all staff, the Bradmas and any other paperwork is returned to the plastic pocket and left in the designated area. (Any paperwork for scanning will be sent after the clinic is finalised)
- At Sunshine: in the PAC tray for completed PACs on wall next to white board.
- At Footscray: in the PAC completed tray on book shelf outside room 2.
Consent
As part of the nursing assessment, PAC nurses will also check that the patient has consent, for the correct procedure, legally correct with all parameters completed, and that the patient understands what procedure they have given consent for. If there are any issues with the consent the PAC Nurse will document this in the Summary section of the Health Questionnaire and/or discuss this with you. It is also the responsibility of the Unit to check Consent validity. That means you must site the waitlist and Consent (AD32) that has been scanned to DMR.
Please ensure you are familiar with the Western Health Consent policy. (Policy code: P-CC3.1) Patients requiring an Interpreter should have the consent co-signed by an independent qualified interpreter. (Procedure code: OP-CM2)
Power of Attorney/Medical Power of Attorney or Public Advocacy should also be noted and copy of paperwork available on DMR. It is also your responsibility to check the details of all Consents on the DMR.
Diabetic patients
All patients with Type 1 DM and Type 2 DM on insulin will require a Diabetic plan for their Insulin. The Unit Doctor can write an AM and a PM admission plan in their PAC note. The patient is given both plans regardless of their admission time. (In case of surgery date/time changes) The advice given for DOS by the nurses will be documented on the top of the Questionnaire in the Summary section (generally, the oral medication advice). The plan should include oral medication advice (if on SGLT2 inhibitor (‘Flozin’), advice as per guidelines), plus the Insulin plan (as per guidelines)
HbA1c
HbA1c must be less than 8% to proceed with non-urgent surgery (18/08/23)
If HbA1c ≥8% defer non-urgent surgery and refer to the Rapid Access Diabetes Clinic (contact Endocrinology Registrar for details) for diabetes optimisation prior to surgery
PAC nursing team will follow up subsequent HbA1c results after Rapid Access Diabetes Clinic
See ‘Preoperative Diabetic guidelines’
If in doubt, please consult with Anaesthetist in clinic or call Endocrinology for advice.
- Insulin requiring patients booked for Surgery on a PM list will be asked to attend earlier at 0930 hours instead of 12:00. Please remind patient of this if admission time is or maybe for a PM list. Fasting advice is still as per a PM admission.
- If Protophane or anything further is required On Admission, this should be documented as a part of the Insulin Plan– the nurse will write this in the Operation Comments on IPM. The list generated on DOS will show this information.
OSA patients
Check Anaesthetic guidelines as for suitability for Williamstown or Sunbury – Day cases generally OK. All patients with OSA that use CPAP will be asked to bring their machine in on the DOS. If unsure, you can discuss with Anaesthetist. Please see Perioperative Obstructive Sleep Apnoea policy on Preoperative Guidelines. http://inside.wh.org.au/policies-procedures-forms/WHDocuments/Perioperative%20Obstructive%20Sleep%20Apnoea%20(OSA).doc
Patients Requiring Further Investigations and Follow Up
Some patients that come to Pre-Admission require further investigations prior to them being deemed fit to proceed for surgery. Common examples of these are TTE, stress TTE, stress MIBI or RFT.
- Whilst the results require review by an anesthetist, it is generally not necessary for a patient to attend to get these results. Therefore once we have the date of the test and the report is available, we will book an Anaesthetic File Review (ANAES F/R), so that an Anaesthetist can review the results without inconveniencing the patient. The PAC nurses will book this review.
- NOT READY FOR CARE:
On these occasions where testing is required pre-operatively and the surgery cannot proceed without reviewing results first, a Not Ready for Care (NRFC) form (Change to Surgery Status AD32.4) should be completed to alert the Elective Bookings Office of deferral until a specified time. Please complete this form and leave with the patient’s paperwork. The ANUM packing up the clinic will fax this to the Elective Surgery Bookings Office to notify them of deferral. You may also like to liaise with your SLN as well.
- UNIT F/R’s:
A Unit F/R will not be booked where the Unit can follow up after PAC. It is the Unit’s responsibility to check outcomes after PAC e.g. GP follow up, Path results etc. These take up valuable patient appointment slots and are not to be done during PAC time.
- Exceptions will be for those patients needing review in another outpatient clinic not of the home Unit. e.g. Ortho patient needing review in Haematology. In this case, we will book a Unit F/R after the appointment to check the outcome.
- If a patient is being reviewed in their own home unit outpatients, the Unit doctors should be aware to follow up after they have been seen, and liaise with their SLN of any changes, and document on the PAC episode notes as an Addendum. e.g. Ortho patient review with Orthopaedic Consultant regarding which hip to do first. The PAC may have been done for upcoming Left Hip replacement but patient is complaining more about Right hip.
If patient is deferred – Please ensure the patient is aware of the deferral, and document this in your plan.
Anticoagulation
This can be a complex area especially as there often new therapies. Western health has an anticoagulation guideline that is available under Anaesthetic Department on the intranet or discuss with an Anaesthetist. All patients on anticoagulation medication need to be given advice as to whether it must continue or cease preoperatively. This is a medical decision based on a number of factors including reason for initiation, risk of bleeding from the surgical procedure and risk of having a thromboembolic event if the medication was to be ceased. Anaesthetist advice should be sought to ensure safety to cease these medications.
Please refer to the Western Health Guidelines ‘Oral Antiplatelet and Anticoagulant Medications in the Perioperative Period for Adults. http://inside.wh.org.au/policies-procedures-forms/WHDocuments/Oral%20Antiplatelet%20and%20Anticoagulant%20Medications%20in%20the%20Perioperative%20Period%20for%20Adults.doc
- If patients are deemed high risk for a thromboembolic event are on Warfarin, and the procedure being done means that they must stop their medication then they will be given bridging Clexane via the nurses with Hospital in the Home (HITH). HITH paperwork is available to complete in PAC. Please be guided by risk assessment and discussion with Anaesthetist or specialist consultant treating the patient. e.g. Neurologist, Cardiologist. If patient has a date, then you can contact the HITH Nurses as well.
- Patients without a date – HITH paperwork can be done and then completed once a date is given or alternatively the Bookings Office may be in touch with the Unit to complete once the date is given.
Summary of General Information for Doctors attending Pre-Admission Clinics
- Please attend clinics promptly and let Nursing staff know you have arrived.
- Please let the Nursing staff know if you have to leave while a clinic is running.
- Generally, the Pre-Admission nurse will see the patient first and information will be on the EMR PAC Nurse Health Questionnaire & Summary. The Summary will contain the name of the Procedure, Surgery date, Consultant, Consent & Other information including anything that needs addressing e.g. anticoagulation, – and the completed Health Questionnaire. Remember to check this Summary & Questionnaire.
- Please write your own assessment notes and history. Do NOT copy and paste from the nurse’s questionnaire. Please ensure that the information aligns with the questionnaire
- At the end of the clinic, the ANUM packing up the clinic, will summarize anything from your notes .e.g. advice given about anticoagulants etc. Please document anything on the medical PAC Admission notes on EMR.
- Doctors Notes on EMR
Use of the EMR Admission template is the correct template. The correct Naming convention is: PAC UNIT (your Unit) ADMISSION PROCEDURE (what surgery is consented for)
Do not use a Progress note, this is for In-patients. Please familiarise yourself in how to use the correct notehttps://digitalhealth.wh.org.au/wp-content/uploads/2019/06/Pre-Admission-Clinic-JMO-Admission-Note.pdf
- Any follow up notes from PAC from this episode of care is written as an Addendum to the original PAC note. A new note is not required during the same episode of care. This means all the information from that PAC for a specific episode of care will be together on EMR.
- Collect the PAC paperwork (Bradmas & any other paperwork) from the designated PAC Unit collection area/tray in time order of appointment where possible.
- Tick the board once you have collected the paperwork before calling the patient, so we can track which patients are being/have been seen & where the paperwork may be. (‘Pick and Tick’). If multiple Doctors from Unit in PAC, please add your initials as well. Cross through the tick when R/V has been completed.
- If you see a patient out of the appointment time order, please ensure the paperwork is placed in the appropriate collection point for the next consultation in time order, where possible
- For patients seen face to face, please hand back any medication advice sheets to the patient with any changes to their medication regimen for day of surgery or before surgery e.g. anticoagulation advice. These are for patients to take home. Do not place them back with the rest of the paperwork.
- Patient paperwork waiting for Anaesthetic review are to be placed in the appropriate box/tray for the Anaesthetist, for collection in patient’s appointment time order, where possible.
- Ensure the patient has seen all required staff before discharging from clinic. Remember to tell the patient they can leave (or no further calls required) if all staff have done the review.
- Completed paperwork (has seen all staff), are to be placed in the Completed PAC tray at Sunshine next to the white board room 9 & at Footscray in the Completed PAC tray on the bookshelf outside room 2.
- Please remember to write down a surgical Plan for each patient on your notes, include:
1) If they are fit to proceed & suitable campuses (not only where they are booked to)
2) Tests required/requested /reviewed preoperatively and where request slip sent, emailed
if given to patient,
3) Medication advice given,
4) Any further review required and follow up required,
5) Deferred patients – document if patient is aware of deferral and if you have notified the
SLN and complete the NRFC form AD 32.4
If it’s not documented, it isn’t done!
- All baseline pathology ordered is to be competed on the day of PAC attendance where possible (or soon after). Indicate in your plan what tests have been requested. Baseline pathology is valid for 3 months, unless abnormal. If extended G&H is also ordered, please ensure this is within the month before surgery date otherwise it will not be valid. (Extended G&H is valid for one month) Take a clinic list with you, so you can follow up pathology results.
- If a G&H request is given to patients without surgical dates, please indicate on your plan and advise patient to have 2/52 preoperatively when they are given their date by the Elective Surgery Bookings office. (They may also have to fill out the hospital and date section on the form once they know the surgical date/campus or let Pathology collector know) A separate G&H form should be given for these patients.
**G&H are only done at Footscray or Sunshine Pathology.
- Sign off any ECG tracings and ensure no acute changes before discharging patient from clinic, or discuss with Senior colleague or Anaesthetist.
- Please place all paperwork together in plastic pocket when finished.
Any follow ups or outcomes that need to be done outside of the PAC appointment, liaise with your Surgical Liaison Nurse. This includes updates for OPD outcomes, changes fitness to proceed/deferrals etc.
- Exceptions are patients referred to other Outpatient clinics e.g. Neurology. Where an outcome is required, in which case a Unit F/R for outcome of OPD r/v can be made. If reviewing within own Home Unit clinic – any outcomes can be directed to your Surgical Liaison Nurse in Bookings. e.g. deferred, remove from W/List, Proceeding etc. and your episode of care PAC EMR notes can be updated via the Addendum
- Unit F/R will not be booked for normal follow up that the Unit is responsible for: e.g. Path/Unit pre-op specific requirements, clearances from GP – current URTI, Fungal nail etc.
- Any Cardiac or Respiratory Function tests will have an Anaesthetic F/R booked for outcomes. e.g. Echo/Stress Echo/MIBI/RFTs etc. and outcomes relayed to the SLN.
- Patients needing physical review may be rescheduled back to a PAC at a later date or may need to be reviewed back at the Unit Outpatient clinic. PAC is generally not the place to review patients that need Consultant input.
Please keep room tidy and replace any forms in appropriate allocated slot before you leave
and wipe down touch surfaces with Clinell wipes
- Please log off computer when you are finished & shut down the computer at end of p.m. shift. Not just the applications/programs, you must log off the computer. (As per WH policy you must at least log off)
- In charge nurse is in room 2 at Sunshine
- In charge nurse is in room 1 or room 2 at Footscray. Check at start of PAC time.
- Please ask if you are unsure or have any queries. All concerns are to be conveyed to the nurse in charge.
- Sunshine Hospital FAX number is 8345 4325
- Footscray Hospital FAX number is 8345 6686
- For switch board dial 9
- LAN page is available on all Computers.
- Telephone paging dial 62 and follow the prompts
Other Processes
FTA (Fail to Attend) – PAC nursing staff will attempt to contact the patient to ascertain the reason for failing to attend. If possible a Nurse PAC over the phone can be done or patient can be given next PAC appointment available if surgery date allows. In case of multiple FTAs, these will be directed back to the Elective Surgery Bookings Office. In cases where we are unable to contact the patient, it will be re-directed to the Elective Surgery Bookings Office to re-book the PAC when able to contact.
NFRC (Not Ready for Care – Change to Surgery Status AD32.4) – NRFC paperwork should be completed.
- Clinical reasons where patient’s surgery should not proceed or patient is unsuitable for allocated campus and a change of campus is required.
- Complete paperwork with reason and management plan and resume/ review date e.g. TTE & r/v of results. Include TTE appointment date & Anaes F/R post TTE
- Personal Reasons, needs to be within their Category timeframe. e.g. patient wishes to postpone due to going overseas, resume date is date of return. Ensure that Personal deferrals are within guidelines for Category. e.g. Cat 2 cannot defer for more than total 3 months.
- Previous/multiple Personal reason deferrals, and not accepting surgery date – this may need to be Removed from Waitlist. The patient will need to go through the waitlist process again.
Cardiology Registrar/tech Referral for Implantable Defibrillator deactivation
If patient has not had PPM check within 12 months or AICD check within 6 months and cannot be checked before surgery date by usual provider, a referral to Cardiology Electrophysiology Clinic in OPD is required
Patients with AICD would normally also be seen by Anaesthetist in PAC. If not, please discuss with Anaesthetist.
- Check Pacemaker/ICD guidelines under Anaesthetics Department intranet site: – Clinical guidelines on PPM-ICD http://inside.wh.org.au/departmentsandservices/Anaesthetics/Pages/Preoperative-Guidelines.aspx
- Pre-operative deactivation of an AICD is required – usually Magnet response. Most of these patients would normally have an Anaesthetic r/v. If no Magnet response, they would need a referral for a technician for DOS.
- If PPM/AICD check is urgent, you may need to speak to the Cardiology Registrar to facilitate in the Electrophysiology Clinic (Pacemaker Clinic) or for DOS check.
Hospital in the Home (HITH)
Complete paperwork where HITH referral is required -The Referral, Prescription, Drug chart & Countdown/guideline sheet. Notify HITH. Paperwork goes to HITH. Patient may take Clexane prescription with them if face to face PAC. *Note: if patient takes Prescription, please photocopy these for HITH before patient leaves.
If patient does not have a date yet, you may be asked to do the HITH paperwork by your SLN once a date has been given.
**A Summary Information Sheet for Doctors is located in each consultation room, or speak to the Nurse in charge of the clinic if you have any concerns**
Guidelines for Ordering Basic Pre-op Investigations
Authorship
2023 – Susan Beasley, Phong Tran, Sean Griffiths, Francesca Sasanelli